Section 1: Evaluation of Permanent Physical Impairment
Distinction Between Evaluation of Permanent Disability and Permanent Physical Impairment
The Disability Committee of the American Medical Association (AMA) has pointed out that the evaluation of permanent disability is twofold1:
- The medical evaluation of the permanent physical impairment.
- The rating of the disability according to the administrative bodies.
The AMA Guide further explains that there should be a distinction between the terms, "permanent disability" and "physical impairment," defined as follows:
- "Permanent disability is not a purely medical condition. A patient is ‘permanently disabled’ if ‘under a permanent disability’ when his actual or presumed ability to engage in gainful activity is reduced or absent because of ‘impairment’ and no fundamental or marked change in the future can be expected."
- "Physical impairment is a purely medical condition. Permanent physical impairment is any anatomical or functional abnormality or loss after maximum medical rehabilitation has been achieved and which abnormality or loss the physician considers stable or non-progressive at the time the evaluation is made."
- "The evaluation rating of 'permanent disability' is an administrative, not a medical responsibility and function."
1AMA Guide to the Evaluation of Permanent Impairment, American Medical Association, February 1989.
Definition of Disability
According to Webster's Dictionary, Disability is defined as:
- "State of being disabled; absence of competent physical, intellectual, or moral power, fitness, or the like; also an instance of such lack."
- "Legal incapacity, incompetence, or disqualification."
Medically, disability is physical impairment and inability to perform physical functions normally.
Legally, disability is permanent injury to the body for which the person should or should not be compensated.
Under the statutes of workers' compensation, disability may be divided into three periods - which are:
- Temporary total disability is that period in which the injured person is totally unable to work. During this time he receives medical treatment.
- Temporary partial disability is that period when recovery has reached the stage of improvement so that the person may begin some kinds of gainful employment.
- Permanent disability applies to permanent damage or to loss of use of some part of the body after the stage of maximum improvement from medical treatment has been reached and the condition is stationary.
Section 2: Rating Guide
This section is made available to the physicians of the State of North Carolina as a guide in rating industrial accidents. It has been felt that a reference point was needed by physicians in making impairment evaluations.
This section is intended to be used only as a guide and basic outline for physicians making rating examinations of individuals who have had industrial injuries to their spine or extremities because in many cases there are intangible factors which cannot be stereotyped but must be considered. Among these factors are pain, weakness, and dexterity.
Under the North Carolina workers' compensation law, the physician rates injuries according to percentage of impairment of the affected part. This percentage is then interpolated by the Commission with the value of this part as determined by law and an award given accordingly. It is the physician’s responsibility only to determine what percentage of a given system or member is impaired.
It should be re-emphasized that the following outline is intended to be used only as a guide by physicians in rating persons. The final rating of impairment should be entirely the examining doctor’s independent opinion based on his own knowledge, experience and clinical examination.
Lower Extremities
A. Some Basic Principles for Evaluation of Lower Extremities:
- Where a joint of the lower extremity has reparative, reconstructive surgery and a part of the joint removed or repaired with resultant osteoarthritis or traumatic arthritis anticipated, consider a minimum of 10% impairment of the joint.
- Evaluation of impairment following fractures of the femur and/or the tibia and fibula is done by first evaluating any shortening and assigning impairment resulting from this; then determining the function of the adjacent joints and arriving at the impairment of these joints. The impairment is then the combined total resulting from shortening, deformity, and the impairment of the adjacent joints.
- Malrotation and angulatory deformities that persist following injuries will be considered in evaluation of permanent impairment.
B. Evaluation of Lower Extremity:
- Shortening of Leg
| Shortening | AWW Impairment to Whole Leg |
|---|---|
| 1/2 inch | 4% |
| 1 inch | 8% |
| 1 1/2 inch | 16% |
| 2 inch | 24% |
| 2 1/2 inch | 32% |
| 3 inch | 40% |
- Hip - Percentage of Impairment of Whole Leg
- Ankylosis of the hip in optimum position (in less satisfactory position, appropriately higher percentage) = 50%
- Arthroplasty of hip using prosthesis or cup (optimum results) = 40%
- Limitation of motion of Hip
- Mild Deformity = 15%
- Example: AP motion: between 0 degrees and 80 degrees flexion
- Lateral motion: 15 degrees adduction to 15 degrees abduction
- Rotation: 20 degrees internal to 20 degrees external rotation
- Moderate Deformity = 30%
- Example: AP motion: 20 degrees flexion to 70 degrees flexion
- Lateral motion: 10 degrees adduction to 30 degrees abduction
- Rotation: 0 degrees internal rotation to 20 degrees external rotation
- Severe Deformity = 60%
- Example: AP motion: 30 degrees flexion to 50 degrees flexion
- Lateral motion: 30 degrees adduction to 40 degrees abduction
- Rotation: as much as 10 degrees internal rotation to 30 degrees external rotation
- Mild Deformity = 15%
- Knee - Percentage of Impairment of Whole Leg
- Ankylosis in optimum position (Ankylosis in less favorable position increasing impairment up to 90% with the knee in a non-weight bearing position) = 50%
- Arthroplasty of knee using prosthesis or cup (optimum results) = 40%
- Limitation of motion of Knee
- Motion between 0 degrees to 60 degrees = 30%
- Motion between 0 degrees to 90 degrees = 15%
- Motion between 0 degrees to 110 degrees = 5%
- Motion between 45 degrees to 135 degrees = 45%
- Ankle and Foot - Percentage Impairment of "Foot" (Leg below the Knee)
- Ankylosis of ankle in favorable position (10 to 15 degrees equinus) with normal motion of foot = 40%
- Ankylosis of foot (subtalar) in optimum position with normal ankle motion = 25%
- Ankylosis in less favorable position up to = 90%
- Ankylosis of foot and ankle (pantalar arthrodesis) in favorable position (10 or 15 degrees equinus) in neutral position of foot = 60%
- Limitation of motion of ankle
- Motion between 90 degrees and 120 degrees = 10%
- Motion between 100 degrees and 115 degrees = 25%
- Motion between 105 degrees and 110 degrees = 50%
- Limitation of motion of foot
- Motion of inversion of 20 degrees to eversion of 20 degrees = 10%
- Motion of inversion of 10 degrees to eversion of 10 degrees = 20%
- Motion of inversion of 5 degrees to eversion of 5 degrees = 40%
- Fixed varus position = up to 90%
- Ankylosis of subtalar joint = 25%
- Triple arthordesis of foot = 30%
- Displaced tarsal fractures considered as having a minimum of 5% impairment of the foot with optimum reduction. In the case of this portion of the foot, impairment is determined mainly upon the general position of the longitudinal arch and/or weight bearing position of the metatarsal heads with respect to the transverse arch rather than by evaluation of motion of the adjacent joints.
Upper Extremities
The individual member is to be rated. If damage is limited to the digits distal to the metacarpophalangeal joint, then the digit itself should be rated. If there is anatomical damage proximal to the metacarpophalangeal joint, a rating for the hand should be given, including any consideration for the digit as a percentage of the hand. If anatomical damage includes an area proximal to the elbow joint, the disability rating should be for the arm and include any percentage which would have otherwise been credited for the hand or digits.
A. "Ankylosis" and "Limited Motion with Pain."
- Fingers
- Ankylosis of distal IP joint (in optimum position) = 35% of digit
- Ankylosis of proximal IP joint (in optimum position) = 50% of digit
- Ankylosis of metacarpal-phalangeal joint (in optimum position) = 45% of digit
- Any of the above in malposition = up to 100% of digit
- Wrist
- Ankylosis in optimum position = 35% of "hand"
- Ankylosis in malposition = up to 100% of "hand"
- Limited motion, mild = up to 10% of hand
- moderate = up to 20% of hand
- severe = up to 25% of hand
- Elbow
- Ankylosis in optimum position = 50% of arm
- Ankylosis in malposition = up to 90% (Straightened position not as disabling as marked flexion.)
- Limited motion and pain
- Flexion and extension (accounts for 60% of elbow function.)
- 20º motion in middle range = 35% of "arm" (80 to 100%)
- 40º motion in middle range = 30% of "arm" (70 to 100%)
- 120º motion in middle range = 5% of "arm" (45 to 160%)
- Pronation and Supination account for 40% of elbow function
- Total loss in neutral position = 25% of hand
- 20º motion each way from neutral 20% of hand
- 60º motion each way from neural 5% of hand
- Arthroplasty of elbow using prosthesis = 40% of arm
- Flexion and extension (accounts for 60% of elbow function.)
- Shoulder
- Ankylosis in optimum position = 50% of "arm"
- Ankylosis in malposition = up to 80% of "arm"
- Resection end of clavicle (distal to coranoid and trapezoid ligaments) = 5% plus limitation
B. Fractures
- Fingers and Metacarpals
- Mal-alignment, shortening, stiffening, etc., rated according to function of finger. Express as "percent of digit" if loss is distal to MP joint; otherwise, as "percent of hand," calculated from the sum of each involved digit, reduced to its known percent of hand.
- Carpals
- Rated according to function of wrist.
- Forearm Fractures
- Mal-alignment
- Rated primarily on limited motion in wrist joint. Add for angulation, shortening, weakness, etc.
- Express as "percent of hand." Occasionally the elbow must also be rated for loss of motion, expressed in "percent of the arm" and the total impairment calculated from the sum of the parts reduced to their relative percent of the whole.
- Excision of fractured radial head
- Full motion with no pain = 10% of arm
- Otherwise rate on basis of loss of motion and pain in elbow and wrist.
- Excision of distal end of ulna
- Rated on basis of adjacent joint function with minimum loss of 10% of hand
- Mal-alignment
- Fractures of humerus
- Mal-alignment
- Rated primarily on basis of limited motion and pain in shoulder and elbow joints, and expressed in "percent of arm." Add for angulation, shortening, weaknesses, etc., not reflected in loss of joint function.
- Fractures of shoulder girdle
- Rated according to function of shoulder joint. Add for pain and weakness in non-union.
- Fracture into a joint. In general, add 10% if minimal displacement, and more if joint surface is irregular.
- Any time a joint is entered surgically for repair or excision of a part, the minimum impairment is to be 10%
- Mal-alignment
C. Laceration of the Hand (Tendon, Nerve, Joint, Etc.)
- Loss of sensation (complete and noticeable) (exclusive of tendon damage)
- ½ of distal phalanx = 25% of digit
- ½ of finger = 100% of digit
- Division of flexor sublimis with full extension of finger
- Tendon only = 10% of digit
- Division of flexor profundus
- Tendon only = 75% of digit
- Division of both profundus and sublimis tendons.= 90% of digit
- Arthrodesis of distal IP joint = 35% of joint
- Arthrodesis of proximal IP joint = 50% of digit
- Arthrodesis of MP joint = 45% of digit
- Above ratings are for arthrodesis in optimum position. Add for malposition.
- "Contractures" of joints or "limited motion and pain." Impairment determined on basis of severity as compared to arthrodesis of the joint.
D. Peripheral Nerve Injuries
(Rated on basis of loss in the "hand." If lesion is high and involves structures above biceps insertion, then loss is rated on the "arm.")
- Ulnar nerve injury
- Complete motor and sensory = 60% of "hand"
- Complete motor and partial sensory = 50% of "hand"
- Motor only = 40% of "hand"
- Median nerve injury
- Complete motor and sensory = 90% of "hand"
- Complete motor and partial sensory = 60% of "hand"
- Motor only to thumb = 35% of "hand"
- Radial nerve injury
- Motor and sensory = 75% of "hand"
- Above estimates are given prior to any reconstruction and may be reduced considerably by reconstructive surgery.
- If contracture has occurred in the digits, additional impairment should be added.
Cervical Spine
Note on rating of back injuries: the statutes, as written, refer to the back, not the spine. When rating impairment to the spine, always refer to it as the back (percentage of the back, not percentage of the spine.)
A. Cervical Spine Fractures
- Single, healed, with little or moderate anterior compression and without neurological findings
- Body = 10%
- and/or posterior elements—arch, transverse process (additional) = 5%
- Two or more vertebrae, each additional = 50% of above
- Add, for neurological
- Quadriplegia = 100% of man
- Nerve root, one arm, or both arms: Functional rating is added to cervical spine percentage.
B. Cervical Disc
- Anterior discectomy, with or without fusion—free of neck and arm pain—no weakness = 5%
- Postoperative—with recurrent episodes of significant cervical and arm pain associated with objective findings = 10-15%
- Posterior laminectomy—removal of ruptured disc—free of neck and arm pain—no weakness = 5%
- Postoperative—with recurrent episodes of significant cervical pain associated with objective findings = 10-15%
Thoracic Spine
A. Thoracic Spine Fractures (treat as Cervical Spine, A)
B. Thoracic Disc (rate as Ruptured Lumbar Disc)
Lumbar Spine
A. Lumbar Spine Fractures (including lower three dorsal vertebrae)
- One body = 10%
- and/or posterior elements (arch and/or transverse process) = additional 5%
- (Two or more) = 50% of above
- Add for loss of motion
- Mild (0%-25% limitation) = 5%
- Moderate (25%-50% limitation) = 10%
- Marked (50% or more limitation) = 20%
- Add for neurological changes: (paraplegias are established)
- One or both legs, functional rating.
B. Invertebral Disc (rate as Ruptured Lumbar Discs)
*This Section clarified as of February 15, 2000
If a claimant has two injuries to the back and has separate impairments, these ratings should be calculated separately and then combined. Do not add the percentages of impairment.
First Example: 40% (A) & 20% (B)
In this example, the first percentage of impairment, 40% (A) is subtracted from 100%.
100% - 40% = 60% (C)
The second percentage of impairment 20% (B) is calculated from the remaining percentage (C), which in this case is 60%.
20% of 60% = 12% (D)
The total percentage of impairment is the sum of 40% (A) plus 12% (D).
40% + 12% = 52% total percentage of impairment
Second Example (When total Exceeds 100%): 70% (A) and 40% (B)
In this example, the first percentage of impairment 70% (A) is subtracted from 100%.
100% - 70% = 30% (C)
The second percentage of impairment 40% (B) is calculated from the remaining percentage (C), which in this case is 30%.
40% of 30% = 12% (D)
The total percentage of impairment is the sum of 70% (A) plus 12% (D).
70% + 12% = 82% total percentage of impairment
Example:
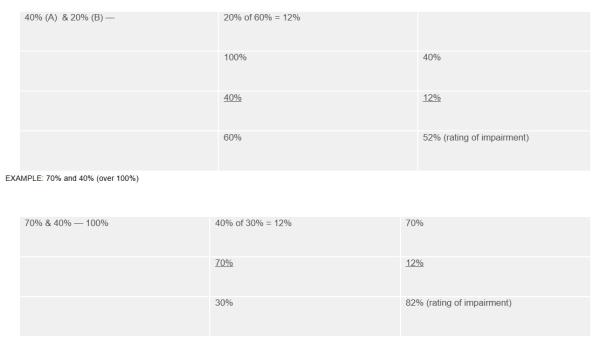
Note: Multiple impairments in the same anatomic region should be combined, not added, as illustrated above.
Pelvis (rate as percentage pf spine unless acetabulum is involved)
A. Symphysis Separation = 10%
B. Ilium
- With pelvic ring intact = 0%
- With pelvic ring displaced 1" or more = 10%
C. Ischium
- Healed, no deformity = 0%
- Healed, deformity and pain = 5-10%
D. Fractured Acetabulum - (evaluate on basis of hip disability-see hip section)
E. Pelvic Ring Displaced Plus Sacroiliac Joint Displaced (if leg shortening, add that) = 15%
Sacrum
- Healed, no pain = 0%
- Healed, with significant residual deformity = 10%
Coccyx
- Healed, no pain = 0%
- Healed, deformity and significant objective signs = 5-10%
- Excised (as above under healed fractures)
Ruptured Lumbar Discs
The following guide is suggested for use in rating of patients with ruptured lumbar discs from the standpoint of permanent partial impairment to the back, as recommended by the North Carolina Orthopaedic Society and the neurosurgeons of North Carolina:
- Typical episode of back and leg pain that completely recovers without neurological defect on conservative therapy = 0%
- Same as (1) with recurrent episodes of significant back pain associated with objective findings = 5-10%
- Postoperative-removal of ruptured disc-free of back and leg pain-no weakness = 5%
- Postoperative-with recurrent episodes of significant back pain associated with objective findings = 10-15%
- Postoperative-removal of ruptured disc and spinal fusion. Same as (3) = 25%
- Postoperative-removal of rupture disc and spinal fusion. Same as (4) = 25-30%
Payments for Scheduled Injuries
Permanent Partial Disability: If, at the end of the healing period, there is a permanent impairment to one of the parts of the body listed below, the employee may receive a set period of benefits without regard to his ability to earn wages. Total loss of use of the part entitles the employee to two-thirds (2/3) of his average weekly wage, times the number of weeks shown following the body part below. Benefits for less than total loss are figured on a percentage basis. For example, twenty percent (20%) of 45 weeks’ compensation is nine (9) weeks. Alternatively, in cases where the employee has a permanent impairment to one of the parts of the body listed below and is unable to earn wages as great as before the injury, the employee may choose to receive benefits for two-thirds (2/3) of the wage difference for a period not to exceed 300 weeks from the date of injury rather than receiving benefits for a set period based on the permanent impairment. The 300-week period, however, will be reduced by the number of weeks Temporary Total Disability Compensation was paid.
The percentage of disability is determined based on physicians’ ratings of the percentage of physical impairment. If there is a dispute between physicians regarding ratings, the Commission will determine the percentage of disability. If either party is dissatisfied with the treating physician’s rating, it may obtain the "second opinion" of another doctor. The employee, upon approval by the Commission, is entitled to a single second opinion rating by a doctor of his or her choice at the employer’s expense. If, however, the employee is unable to earn any wages in any employment, he or she may elect to receive either the carrier’s offer for the rating or for his ongoing disability, whichever remedy provides the most reimbursement.
| Part of Body | Number of Weeks | Part of Body | Number of Weeks |
|---|---|---|---|
| Thumb | 75 Weeks | Arm | 240 Weeks |
| First or index finger | 45 Weeks | Foot | 144 Weeks |
| Second or middle finger | 40 Weeks | Leg | 200 Weeks |
| Third or ring finger | 25 Weeks | Eye | 120 Weeks |
| Fourth or little finger | 20 Weeks | Hearing (one ear) | 70 Weeks |
| Great toe | 35 Weeks | Hearing (both ears) | 70 Weeks |
| Any other toe | 10 Weeks | Back | 150 Weeks |
| Hand | 200 Weeks |
If the injury results in amputation or permanent total loss of a specific member, compensation is payable at the end of the healing period during the number of weeks set forth in the table.
If the injury results in only partial amputation or loss of use of a particular member, compensation is paid on a percentage basis. For example, if the injury results in 20% permanent partial loss of use of the index finger, the employee is entitled to 20% of 45 weeks of compensation, or 9 weeks.
Computation of Compensation for Amputations
- Amputation of any portion of the bone of a distal phalange of a finger or toe at or distal to the visible base of the nail will be considered as equivalent to the loss of one-fourth (1/4) of such finger or toe.
- Amputation of any portion of the bone of the distal phalange of a finger or toe proximal to the visible base of the nail will be considered as equivalent to the loss of one-half (1/2) of such finger of toe.
- Amputation through the forearm at a point so distal to the elbow as to permit satisfactory use of a prosthetic appliance with retention of full natural elbow function shall be considered amputation of the hand. Otherwise, it shall be considered amputation of the arm.
- Amputation through the lower leg at a point so distal to the knee as to permit satisfactory use of a prosthetic appliance with retention of full natural knee function shall be considered amputation of the foot. Otherwise, it shall be considered amputation of the leg.
See N.C. Gen. Stat. §97-31 for more information.
Loss of Vision
Note: Loss of vision must be based upon the reading without the use of a corrective lens.
The Loss of Vision table, according to the Snellen Notation, is the one used by the North Carolina Industrial Commission for determining the percentage of loss of vision. Loss in muscle function or visual field may in conjunction with other factors indicate a greater percentage of loss vision.
"… in cases where there is 85 per centum, or more, loss of vision in any eye, this shall be deemed ‘industrial blindness’ and compensates as for total loss of vision of such eye." N.C. Gen. Stat. §97-31(19).
Disfigurement Involving Loss of Permanent Teeth and Teeth Restored with Crowns
In workers’ compensation cases where the teeth are extracted due to an accidental injury, the full disfigurement amount will be paid. If the teeth are crowned, 50% of the value of the tooth will be allowed. If the tooth is merely chipped and a cap-type repair is done, then, of course, no compensation would be paid for disfigurement. In addition to any disfigurement due, all medical bills will be paid after being submitted to the Commission and approved by the medical fee schedule.
The following guideline will be used in approving agreements for disfigurement due to the loss of permanent teeth.
| Age | Amount of Tooth | Crown (50%) |
|---|---|---|
| up to 23 | $720.00 | $360.00 |
| 24-26 | $600.00 | $300.00 |
| 27-29 | $540.00 | $270.00 |
| 30 and over | $420.00 | $210.00 |
The above applies to injuries occurring on and after January 1, 1996.
N.C. Gen. Stat. §97-53 Occupational Diseases Enumerated; When Due to Exposure to Chemicals
The following diseases and conditions only shall be deemed to be occupational diseases within the meaning of this N.C. Gen Stat. §97-53:
- Anthrax.
- Arsenic poisoning.
- Brass poisoning.
- Zinc poisoning.
- Manganese poisoning.
- Lead poisoning. Provided the employee shall have been exposed to the hazard of lead poisoning for at least 30 days in the preceding 12 months’ period; and, provided further, only the employer in whose employment such employee was last injuriously exposed shall be liable.
- Mercury poisoning.
- Phosphorous poisoning.
- Poisoning by carbon bisulphide, menthanol, naphtha or volatile halogenated hydrocarbons.
- Chrome ulceration.
- Compressed-air illness.
- Poisoning by benzol, or by nitro and amido derivatives of benzol (dinitrolbenzol, anilin, and others).
- Any disease, other than hearing loss covered in another subdivision of this section, which is proven to be due to causes and conditions which are characteristic of and peculiar to a particular trade, occupation or employment, but excluding all ordinary diseases of life to which the general public is equally exposed outside of the employment.
- Epitheliomatous cancer or ulceration of the skin or of the corneal surface of the eye due to tar, pitch, bitumen, mineral oil, or paraffin, or any compound, product, or residue of any of these substances.
- Radium poisoning or disability or death due to radioactive properties of substances or to roentgen rays, X rays or exposure to any other source of radiation; provided, however, that the disease under this subdivision shall be deemed to have occurred on the date that disability or death shall occur by reason of such disease.
- Blisters due to use of tools or appliances in the employment.
- Bursitis due to intermittent pressure in the employment.
- Miner’s nystagmus.
- Bone felon due to constant or intermittent pressure in employment.
- Synovitis, caused by trauma in employment.
- Tenosynovitis, caused by trauma in employment.
- Carbon monoxide poisoning.
- Poisoning by sulphuric, hydrochloric or hydrofluoric acid.
- Asbestosis.
- Silicosis.
- Psittacosis.
- Undulant fever.
- Loss of hearing caused by harmful noise in the employment. The following rules shall be applicable in determining eligibility for compensation and the period during which compensation shall be payable:
- The term "harmful noise" means sound in employment capable of producing occupational loss of hearing as hereinafter defined. Sound of an intensity of less than 90 decibels, A scale, shall be deemed incapable of producing occupational loss of hearing as defined in this section.
- "Occupational loss of hearing" shall mean a permanent sensorineural loss of hearing in both ears caused by prolonged exposure to harmful noise in employment. Except in instances of preexisting loss of hearing due to disease, trauma, or congenital deafness in one ear’, no compensation shall be payable under this subdivision unless prolonged exposure to harmful noise in employment has caused loss of hearing in both ears as hereinafter provided.
- No compensation benefits shall be payable for temporary total or temporary partial disability under this subdivision and there shall be no award for tinnitus or a psychogenic hearing loss.
- An employer shall become liable for the entire occupational hearing loss to which his employment has contributed, but if previous deafness is established by a hearing test or other competent evidence, whether or not the employee was exposed to harmful noise within six months preceding such test, the employer shall not be liable for previous loss so established, nor shall he be liable for any loss for which compensation has previously been paid or awarded and the employer shall be liable only for the difference between the percent of occupational hearing loss determined as of the date of disability as herein defined and the percentage of loss established by the preemployment and audiometric examination excluding, in any event, hearing losses arising from nonoccupational causes.
- In the evaluation of occupational hearing loss, only the hearing levels at the frequencies of 500, 1,000, 2,000 and 3,000 cycles per second shall be considered. Hearing losses for frequencies below 500 and above 3,000 cycles per second are not to be considered as constituting compensable hearing disability.
- The employer liable for the compensation in this section shall be the employer in whose employment the employee was last exposed to harmful noise in North Carolina during a period of 90 working days or parts thereof, and an exposure during a period of less than 90 working days or parts thereof shall be held not to be an injurious exposure; provided, however, that in the event an insurance carrier has been on the risk for a period of time during which an employee has been injuriously exposed to harmful noise, and if after insurance carrier goes off the risk said employee has been further exposed to harmful noise, although not exposed for 90 working days or parts thereof so as to constitute an injurious exposure, such carrier shall nevertheless, be liable.
- The percentage of hearing loss shall be calculated as the average, in decibels, of the thresholds of hearing for the frequencies of 500, 1,000, 2,000, and 3,000 cycles per second. Pure tone air conduction audiometric instruments, properly calibrated according to accepted national standards such as American Standards Association, Inc., (ASA), International Standards Organization (ISO), or American National Standards Institute, Inc., (ANSI), shall be used for measuring hearing loss. If more than one audiogram is taken, the audiogram having the lowest threshold will be used to calculate occupational hearing loss. If the losses of hearing average 15 decibels (26 db if ANSI or ISO) or less in the four frequencies, such losses of hearing shall not constitute any compensable hearing disability. If the losses of hearing average 82 decibels (93 db if ANSI or ISO) or more in the four frequencies, then the same shall constitute and be total or one hundred percent (100%) compensable hearing loss. In measuring hearing impairment, the lowest measured losses in each of the four frequencies shall be added together and divided by four to determine the average decibel loss. For each decibel of loss exceeding 15 decibels (26 db if ANSI or ISO) an allowance of one and one-half percent (1½%) shall be made up to the maximum of one hundred percent (100%) which is reached at 82 decibels (93 db if ANSI or ISO). In determining the binaural percentage of loss, the percentage of impairment in the better ear shall be multiplied by five. The resulting figure shall be added to the percentage of impairment in the poorer ear, and the sum of the two divided by six. The final percentage shall represent the binaural hearing impairment.
- There shall be payable for total occupational loss of hearing in both ears 150 weeks of compensation, and for partial occupational loss of hearing in both ears such proportion of these periods of payment as such partial loss bears to total loss.
- No claim for compensation for occupational hearing loss shall be filed until after six months have elapsed since exposure to harmful noise with the last employer. The last day of such exposure shall be the date of disability. The regular use of employer-provided protective devices capable of preventing loss of hearing from the particular harmful noise where the employee works shall constitute removal from exposure to such particular harmful noise.
- No consideration shall be given to the question of whether or not the ability of an employee to understand speech is improved by the use of a hearing aid. The North Carolina Industrial Commission may order the employer to provide the employee with an original hearing aid if it will materially improve the employee’s ability to hear.
- No compensation benefits shall be payable for the loss of hearing caused by harmful noise after October 1, 1971, if employee fails to regularly utilize employer-provided protection device or devices, capable of preventing loss of hearing from the particular harmful noise where the employee works.
Occupational diseases caused by chemicals shall be deemed to be due to exposure of an employee to the chemicals herein mentioned only when as a part of the employment such employee is exposed to such chemicals in such form and quantity, and used with such frequency as to cause the occupational disease mentioned in connection with such chemicals. (1935, c. 123; 1949, c. 1078; 1953, c. 11 12; 1955, c. 1026, s. 10; 1957, c. 1396, s. 6; 1963, c. 553, s. 1; c. 965; 197 1, c. 547, s. 1; c. II 108, s. 1; 1973, c. 760, ss. 1, 2; 1975, c. 718, s. 4; 1987, c. 729, ss. 11, 12; 1991, c. 703, s. 10.)
Summary
The Commission’s rules provide that no case may be settled by compromise settlement agreement unless it is provided that the defendant employer or insurance carrier involved pay all medical bills incurred by the injured employee to date of the settlement agreements, in amounts approved by the Commission in accordance with this fee schedule.
If a physician is dissatisfied with the fee approved for him in a given case, he may ask for a review of his charges by the Medical Fee Committee of the Industrial Committee. The names of the members of this committee may be obtained by writing the N.C. Industrial Commission. In some instances the Commission’s Medical Department will refer a bill to this committee for advice and guidance before any approval.
Any person desiring review of an approval, a failure to approve, or reduction of any fee may request a hearing before the Commission. Such hearing is ordinarily conducted in the county where the accident giving rise to the claim occurred. Such hearing is conducted by a Hearing Commissioner or Deputy Commissioner who makes a decision in the case on the basis of the evidence presented and the applicable law. Such decision may be appealed to and reviewed by the full Commission and by the North Carolina Court of Appeals. Further review may be had in some instances by the North Carolina Supreme Court.
Section 3: Recent Topics of Physician Inquiry
The following are general comments on subjects frequently raised in physicians’ questions addressed to the Commission in recent months.
Rating and Release
Perhaps the most dramatic change in our compensation system in recent years permits a worker to continue receiving benefits if some residual disability prevents him from actually getting and keeping a job, regardless of whether or not he has reached "maximum medical improvement". Thus, it is becoming more common for the claimant and employer to litigate whether or not the claimant is capable of doing a given available job. Your ratings and specific descriptions of physical limitations can be extremely important in a number of contexts. An opinion that the worker is capable of returning to his former employment should be based in part on a specific description of the physical requirements of that job.
A rating is appropriate at the end of the healing period, even though the patient may have earlier progressed to the point that invasive or active treatment is no longer indicated. The ratings in this guide were devised by North Carolina physicians specifically for use with our statute. An AMA "whole person" ratings cannot be readily translated to fit our system.
Second Opinion
The worker is entitled to a second medical opinion, at the employer/carrier’s expense, when he is rated or released. It is not uncommon for employers and carriers to also seek a second opinion on a rating. On relatively rare occasions, most often involving an unrepresented plaintiff, the Commission will order an independent examination or evaluation to help resolve a medical issue. In the context of the legal controversy, the second opinion can be a very valuable item of evidence whether it confirms, adds to or controverts medical evidence already available to us. We urge you to favorably consider these requests and help to insure that these opinions are representative of the medical community.
Medical Records
Both the patient or his authorized counsel and the employer or his insurance carrier are entitled to obtain medical rehabilitation records and the testimony and opinions of those treating the patient as a matter of course. The Commission rules provide that these parties can obtain such records in the others’ possession, without charge. Otherwise, the normal rules of privilege and privacy apply.
When the parties contest whether the injury occurred under compensable circumstances, the history and patient notes taken by the treating physician are frequently critical items of evidence. While it is sometimes inconsequential to determine treatment, a clear record of plaintiffs account of how the symptoms arose can prevent litigation or lead to its early resolution.
Office notes that clearly record the information referred to above can frequently be taken into evidence in lieu of a deposition of the physician.
Rehabilitation Personnel
Insurance carriers are utilizing rehabilitation nurses or specialists with much greater frequency than in years past to monitor the patient treatment and recovery, aid in obtaining compliance with appointments and prescribed treatments, and to facilitate the patient’s return to a job they can perform without inordinate risk to their health. The Workers' Compensation Act provides for their services, as a part of the effort to "effect a cure or give relief and ... lessen the period of disability."
The Commission has received numerous complaints, many from physicians, that rehabilitationists have engaged in activities inconsistent with its role. The services described above are the sole justification for their contact with the represented worker out of the presence of his attorney. The rehabilitationist should not behave during such contacts like an opposing attorney or adjuster. In no instance is the rehabilitationist entitled to direct treatment or substitute their judgment for that of the treating physician. The employer or his carrier is entitled to direct the plaintiff to obtain treatment from another physician if the employer disagrees with the treatment being rendered. However, the worker can apply to the Commission to decide who should be the treating physician, and the Commission will make its decision based on the weight of the medical evidence presented.
It has become common practice for the rehabilitationists to request the opportunity to be present at examinations, and in some instances, present in the examination room. The law requires only that the treating physician admit "a duly qualified physician or surgeon" attending at the request of either the worker or the employer/carrier. However, the Commission encourages all reasonable methods of sharing accurate information in order to facilitate the resolution of claims without litigation and delay.
In any event, the attending physician is in charge of the medical services to be provided for the worker/claimant, and may remove a rehabilitationist from further involvement with medical treatment for the worker/claimant so long as such physician is the attending physician.
Preexisting Infirmity
When an injury occurs due to a worker’s idiopathic condition, it is not compensable. However, if hazards incident to the employment contribute in some definite, discernible way to the cause of the accident, the employer may be liable. If a compensable injury materially accelerates or aggravates a preexisting disease or infirmity and contributes to death or injury, it is compensable even if it would not have caused death or disability to a normal person.
Inquiries
The members of the Industrial Commission are administrators, as well as quasi-judicial officials and education is part of our mission. While we cannot give opinions on specific legal issues in pending cases, we will be glad to assist you with general advice about re-occurring problems that you encounter in seeking to treat the injured worker.